

De Quervain's Syndrome
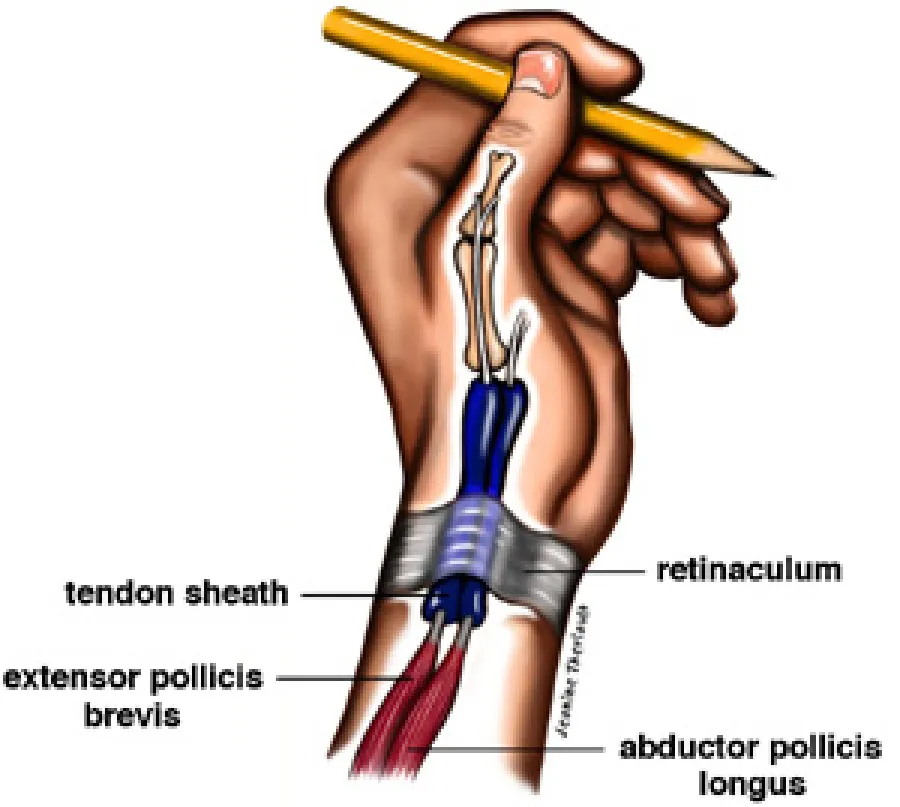
This condition consists of a tenosynovitis of the first dorsal compartment. Within this compartment at the wrist is contained the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendons. It is manifested by pain at the base of the thumb that migrates up the wrist and forearm. It gets worse with thumb movement or grip. It is especially bothersome when trying to open large-mouth jars such as pickles. The pain is crescendo in nature often precluding the ability to continue to hold the object.

Cause
Diagnosis
The history and physical exam is crucial in making this diagnosis as several other conditions may mimic this syndrome. The history is usually one of chronically increasing pain at the wrist that migrates into the thumb and forearm. On exam, localized tenderness will be palpable over the wrist where the tendons cross under the extensor retinaculaum into their tunnel. There are 6 tunnels on the backside of the wrist (dorsal). The tunnel involved will be the first dorsal compartment. A sensitive test is the Finklestein Test in which the fingers grip the thumb, and then the whole wrist is ulnar deviated (pushed toward the little finger). Pain on resisted thumb extension or abduction can also be seen. X-rays are usually not indicated.
Treatment
Conservative treatment is usually begun with splinting the wrist and thumb. (Please note; a carpal tunnel splint does NOT adequately immobilize the thumb).
Non-steroidal anti-inflammatory drugs (NSAID's) are utilized to reduce the inflammation. On occasion, your Orthopedic Surgeon may inject a steroid solution into the first dorsal compartment. If symptoms persist your surgeon may recommend a surgical procedure. In this 10-minute procedure, the roof of the tunnel is released, allowing the tendons to glide freely. A splint is applied that allows movement at the tip of the thumb to keep the tendons gliding. Usually the patient returns to full activities at two weeks post-operatively.

Trivia
Fritz de Quervain first described this syndrome in 1895. He was a distinguished general surgeon who was Professor of Surgery at Berne, Switzerland. He was born at Sion in the Valais Canton of Switzerland, where his dad was the pastor. After his surgical training he settled in the watch-making district of La Chaux-de-Fonds. He worked extensively on Thyroid Goiter and is responsible for the introduction of iodized table salt to help prevent goiter. Initially this tenosynovitis syndrome was thought due to tuberculosis.
Resources
- Olecranon Bursitis
- Osteochondritis Dissecans (OCD)
- Patellofemoral Syndrome
- Plantar Fascitis (Heel Spurs)
- Ruptures Of The Achilles Tendon
- Shoulder Impingement, Bursitis & Tendonitis
- Shoulder Instability
- Shoulder Pain
- Stingers
- Tendonitis (Tennis Elbow)
- Total Knee Replacement
- Trigger Finger
- Total Hip Replacement